This was sent by an anonymous paramedic.
"One of the paramedics at my work approached me the other day and asked for my opinion on two ECGs from a 50s male with sharp chest pain radiating to the back."
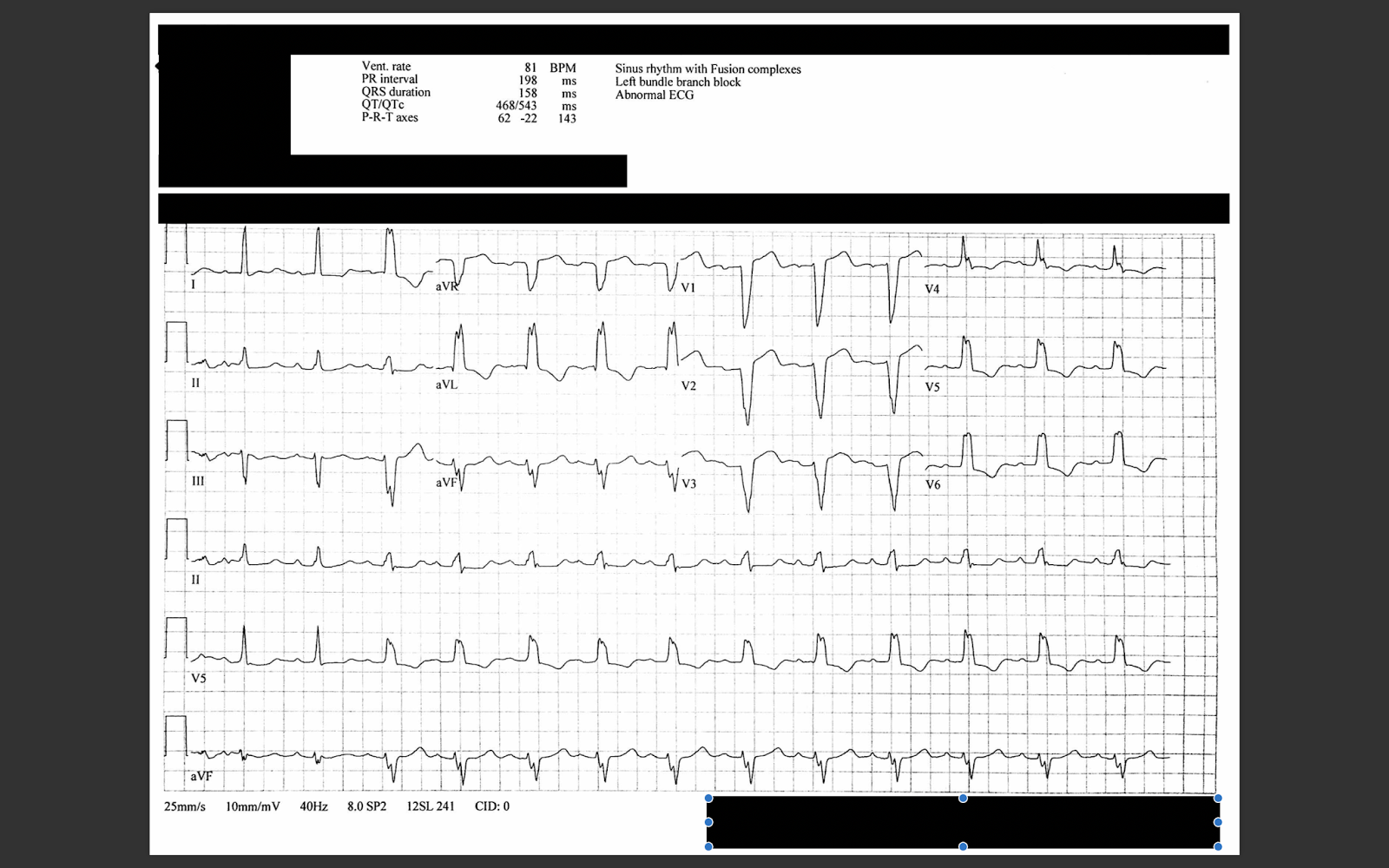
The medic asked for my opinion: "This is diagnostic of LAD occlusion, either mid or distal."
Paramedic thoughts: "I was concerned with the size of the T-waves in V4-V6 and of the STD in the inferior leads with slight STE in aVL."
Smith comment: These T-waves in V4-V6 are all but diagnostic for being hyperacute. When you combine this finding with the STE in I and aVL and the reciprocal ST depression in III, this is diagnostic of coronary occlusion.
See this post:
Paramedic continues: "Although your formula differentiating normal ST elevation from LAD occlusion should not be applied due to the ST Depression in leads II, III, and aVF, I decided to apply both formulas for the fun of it with the following values:"
Note from Smith: the formulas really are intended to differentiate STE in V2-V4 that is normal from that which is due to occlusion. This ECG does not have any appreciable STE in V2-V4. The leads in question are V4-V6 and only because of T-waves, not ST elevation.
Paramedic continues
"For ECG 1: Computerized QTc: 394ms, STEV360ms: 0. R-wave V4: 4mm. QRSV2: 5mm. This received a positive 4-Variable value of 18.66."
"For ECG 2: Computerized QTc: 404ms, STEV360ms: 0. R-wave V4: 2mm. QRSV2: 5mm. This received a negative 3-Var Value of 23.18, and a positive 4-Var Value of 19.72"
The medic recorded another ECG 21 minutes later:
Paramedic: "The ED that this patient was transported to almost never looks at pre-hospital ECGs unless transmitted prior to patient arrival (this one was not), so it is almost guaranteed that the findings would not be appreciated by the receiving physician."
"Anyway, after expressing the concerns that I had, the paramedic told me that the patient waited 90 minutes in the ED prior to being sent to the cath lab. (I did not ask, but I’m assuming that either troponin or serial ECG changes were responsible for the activation)."
Outcome:
"100% LAD occlusion stented. Patient is doing well. If I remember correctly, it was mid-LAD."
This comment is gratifying:
"On another note, I have been following this blog for just over a year now and I can say, without doubt, that i would have missed the subtle findings had it not been for your invaluable knowledge. For that, I sincerely thank you."
"One of the paramedics at my work approached me the other day and asked for my opinion on two ECGs from a 50s male with sharp chest pain radiating to the back."
 |
| What do you think? |
The medic asked for my opinion: "This is diagnostic of LAD occlusion, either mid or distal."
Paramedic thoughts: "I was concerned with the size of the T-waves in V4-V6 and of the STD in the inferior leads with slight STE in aVL."
Smith comment: These T-waves in V4-V6 are all but diagnostic for being hyperacute. When you combine this finding with the STE in I and aVL and the reciprocal ST depression in III, this is diagnostic of coronary occlusion.
See this post:
Ten cases of hyperacute T-waves in V4-V6
Paramedic continues: "Although your formula differentiating normal ST elevation from LAD occlusion should not be applied due to the ST Depression in leads II, III, and aVF, I decided to apply both formulas for the fun of it with the following values:"
Note from Smith: the formulas really are intended to differentiate STE in V2-V4 that is normal from that which is due to occlusion. This ECG does not have any appreciable STE in V2-V4. The leads in question are V4-V6 and only because of T-waves, not ST elevation.
Paramedic continues
"For ECG 1: Computerized QTc: 394ms, STEV360ms: 0. R-wave V4: 4mm. QRSV2: 5mm. This received a positive 4-Variable value of 18.66."
"For ECG 2: Computerized QTc: 404ms, STEV360ms: 0. R-wave V4: 2mm. QRSV2: 5mm. This received a negative 3-Var Value of 23.18, and a positive 4-Var Value of 19.72"
The medic recorded another ECG 21 minutes later:
 |
| No great change |
Paramedic: "The ED that this patient was transported to almost never looks at pre-hospital ECGs unless transmitted prior to patient arrival (this one was not), so it is almost guaranteed that the findings would not be appreciated by the receiving physician."
"Anyway, after expressing the concerns that I had, the paramedic told me that the patient waited 90 minutes in the ED prior to being sent to the cath lab. (I did not ask, but I’m assuming that either troponin or serial ECG changes were responsible for the activation)."
Outcome:
"100% LAD occlusion stented. Patient is doing well. If I remember correctly, it was mid-LAD."
This comment is gratifying:
"On another note, I have been following this blog for just over a year now and I can say, without doubt, that i would have missed the subtle findings had it not been for your invaluable knowledge. For that, I sincerely thank you."