Two Histories, One ECG
Story number one:
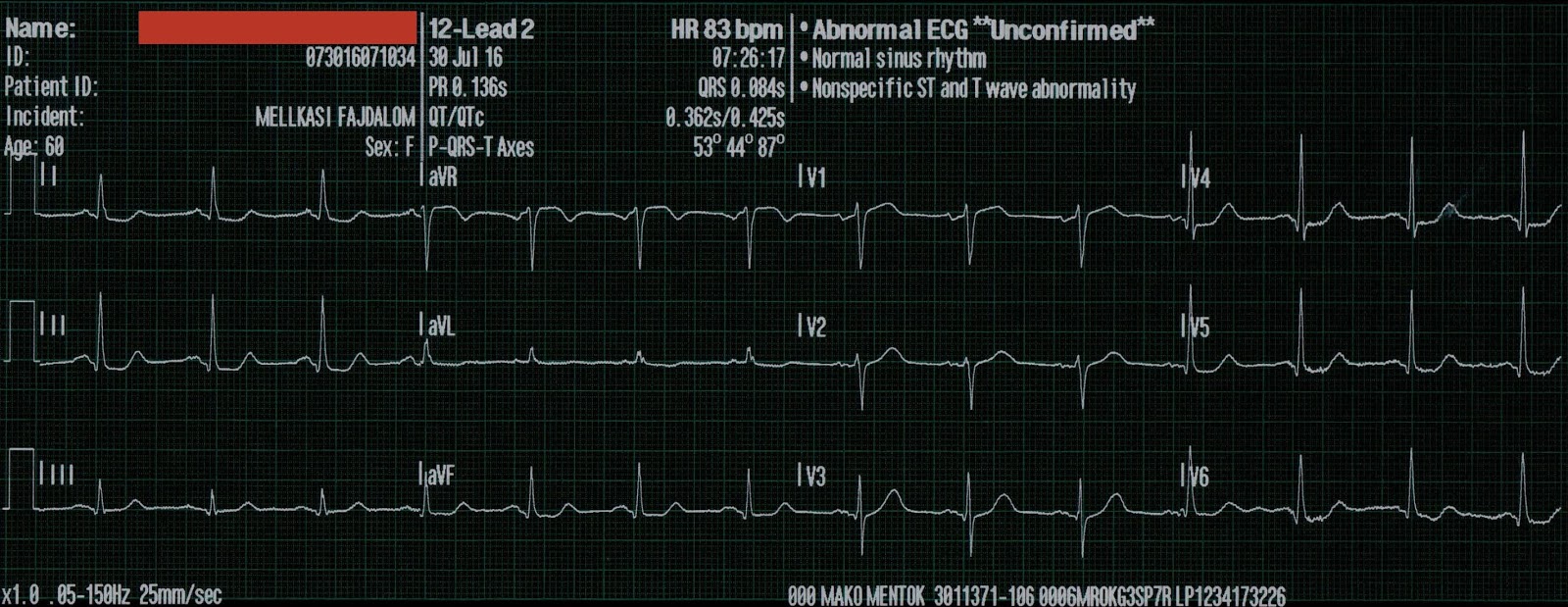
An athletic 20-something presents with chest pain and has this ECG at triage:
In a 20-something, this is a tough ECG. Is it anterior MI?
Being young does not rule it out:
There is sinus bradycardia at a rate of 44.
There is 2 mm of ST elevation in V2 and V3 (at the J-point, relative to the PQ junction), which is below the "criteria" for men under 40 (2.5 mm).
There is upward concavity
There is no ST depression
There are no Q-waves
There is no terminal QRS distortion
So early repolarization is a possibility.
However, there is very suspicious STE in III and aVF, with ST depression in aVL. To me, this makes the ECG nearly diagnostic of ischemia, though if it is LAD occlusion, there should be ST depression in III and aVL, so it is a bit confusing. Unless you consider a wraparound LAD.
There is also an upright T-wave in V1, larger than V6. This is a very soft sign of LAD occlusion, and did not add any diagnostic improvement over our formula model for diagnosing LAD occlusion vs. early repol. In that study, this finding was present in 39% of LAD occlusion and 15% of early repol.
What do the formulas have to add?
Computerized QTc
RAV4 = R-wave amplitude in lead V4
STE60V3 = ST Elevation relative to the PQ jct at 60 ms after the J-point
QRSV2 = total QRS amplitude (Q, R, and S) in lead V2
The 3-variable formula is:
(1.196 x STE at 60 ms after the J-point in V3 in mm) + (0.059 x computerized QTc) - (0.326 x R-wave Amplitude in V4 in mm).
The 4-variable formula is:
(1.062 x STE at 60 ms after the J-point in V3 in mm) + (0.052 x computerized QTc) - (0.151 x QRSV2) - (0.268 x R-wave Amplitude in V4 in mm).
In its derivation study, the 4-variable formula performed better than the 3-variable formula, with an AUC of 0.9538 vs. 0.9686, and was both more sensitive and specific.
http://hqmeded-ecg.blogspot.com/p/rules-equations.html
The measurements are:
RA V4 = 6.5
STE60V3 = 3.0
QRSV2 = 12.5
QTc = 362 ms
The formula values are thus:
3-variable: 22.83 (less than 23.4; the most accurate, but not most sensitive, cutoff). I still worry when the value is above 22.0 (still misses 4% of LAD occlusion when below 22.0)
4-variable 18.38 (greater than 18.2; the most accurate, but not most sensitive, cutoff). So this is strongly indicative of LAD occluson.
Computerized QTc = 362 ms (this is VERY short for LAD occlusion, but is so short because of correction for slow heart rate; the measured QT was 413 ms.) This is the main reason the formula value is not very high.
Thus, the ECG is early repolarization by the old formula and is LAD occlusion by the new one.
Even though the ST Elevation is not diagnostic, and T-waves of this size can be seen in early repolarization, but low QRS and R-wave amplitude is not.
The inferior ST findings also make this ECG diagnostic.
In case you were wondering about the T-waves and bradycardia, the K was normal.
Why bradycardia? Think about that inferior ST elevation. Maybe there is also inferior MI from wraparound LAD with associated sinus bradycardia.
Story number 2: the real story
I was at triage when a 60-something man who had history of elevated cholesterol and hypertension appeared, clutching his chest, diaphoretic and pale, stating he had had sudden onset of substernal CP 30 minutes prior.
I looked at him and thought to myself: "this man is having an anterior MI". I almost activated the cath lab without an ECG, but we recorded one within 1 minute of arrival.
Here is that same ECG again:

I actually only saw lead V2 on the screen of the machine when I activated the cath lab. It had not yet even been printed out.
14 minutes later, just before going to the cath lab, the patient's pain went from 10/10 to 7/10.
Another ECG was recorded:
The patient went to the cath lab:
A large proximal LAD thrombus with TIMI-1 flow was found. Thus, there had been some minimal spontaneous reperfusion (autolysis). It was a wraparound LAD, explaining the inferior ST elevation with reciprocal ST depression in aVL (the opposite of what you expect with a proximal LAD occlusion). It was stented.
The post-cath ECG is here:
The cardiologists were not impressed by the ECG. This is the cardiology note:
"Pt's ECGs were not convincing but presentation was extremely concerning for ACS."
Summary
So this was an anterior and inferior STEMI due to an LAD that wraps around to the inferior wall. We do not see evidence of the ischemia of the first diagonal (which is distal to the occlusion and usually is revealed by STE in I and aVL). This is because that STE was cancelled out by reciprocal ST depression due to the inferior STE. The sinus bradycardia may be due to the inferior wall ischemia, although this happens primarily when there is occlusion of the RCA.
The 4-variable formula was correct.
The door to balloon time was 57 minutes.
This was recorded the next day:
Peak cTnI = 51 ng/mL
The echo next day showed:
The estimated left ventricular ejection fraction is 63 %.
Regional wall motion abnormality-distal septum anterior and apex akinetic
Regional wall motion abnormality-distal inferior wall .
Left ventricular hypertrophy concentric .
Regional wall motion abnormality-anterior akinetic.
Learning Points:
1. The pretest probability is important
2. R-wave amplitude is important
3. The 4 - variable formula is more accurate than the 3-variable
4. Look at the inferior leads.
5. Remember that a wraparound LAD can hide the findings of a proximal occlusion.
Story number one:
An athletic 20-something presents with chest pain and has this ECG at triage:
 |
| QTc = 362 ms What do you think? |
In a 20-something, this is a tough ECG. Is it anterior MI?
Being young does not rule it out:
An intoxicated, agitated, 20-something with chest pain
There is sinus bradycardia at a rate of 44.
There is 2 mm of ST elevation in V2 and V3 (at the J-point, relative to the PQ junction), which is below the "criteria" for men under 40 (2.5 mm).
There is upward concavity
There is no ST depression
There are no Q-waves
There is no terminal QRS distortion
So early repolarization is a possibility.
However, there is very suspicious STE in III and aVF, with ST depression in aVL. To me, this makes the ECG nearly diagnostic of ischemia, though if it is LAD occlusion, there should be ST depression in III and aVL, so it is a bit confusing. Unless you consider a wraparound LAD.
There is also an upright T-wave in V1, larger than V6. This is a very soft sign of LAD occlusion, and did not add any diagnostic improvement over our formula model for diagnosing LAD occlusion vs. early repol. In that study, this finding was present in 39% of LAD occlusion and 15% of early repol.
What do the formulas have to add?
Computerized QTc
RAV4 = R-wave amplitude in lead V4
STE60V3 = ST Elevation relative to the PQ jct at 60 ms after the J-point
QRSV2 = total QRS amplitude (Q, R, and S) in lead V2
The 3-variable formula is:
(1.196 x STE at 60 ms after the J-point in V3 in mm) + (0.059 x computerized QTc) - (0.326 x R-wave Amplitude in V4 in mm).
The 4-variable formula is:
(1.062 x STE at 60 ms after the J-point in V3 in mm) + (0.052 x computerized QTc) - (0.151 x QRSV2) - (0.268 x R-wave Amplitude in V4 in mm).
In its derivation study, the 4-variable formula performed better than the 3-variable formula, with an AUC of 0.9538 vs. 0.9686, and was both more sensitive and specific.
Driver BE and Smith SW: A new 4-variable formula to differentiate normal variant ST segment elevation in V2-V4 (early repolarization) from subtle left anterior descending coronary occlusion - Adding QRS amplitude of V2 improves the model
Both formulas can be calculated at this link on an excel applet:http://hqmeded-ecg.blogspot.com/p/rules-equations.html
The measurements are:
RA V4 = 6.5
STE60V3 = 3.0
QRSV2 = 12.5
QTc = 362 ms
The formula values are thus:
3-variable: 22.83 (less than 23.4; the most accurate, but not most sensitive, cutoff). I still worry when the value is above 22.0 (still misses 4% of LAD occlusion when below 22.0)
4-variable 18.38 (greater than 18.2; the most accurate, but not most sensitive, cutoff). So this is strongly indicative of LAD occluson.
Computerized QTc = 362 ms (this is VERY short for LAD occlusion, but is so short because of correction for slow heart rate; the measured QT was 413 ms.) This is the main reason the formula value is not very high.
Thus, the ECG is early repolarization by the old formula and is LAD occlusion by the new one.
Even though the ST Elevation is not diagnostic, and T-waves of this size can be seen in early repolarization, but low QRS and R-wave amplitude is not.
The inferior ST findings also make this ECG diagnostic.
In case you were wondering about the T-waves and bradycardia, the K was normal.
Why bradycardia? Think about that inferior ST elevation. Maybe there is also inferior MI from wraparound LAD with associated sinus bradycardia.
Story number 2: the real story
I was at triage when a 60-something man who had history of elevated cholesterol and hypertension appeared, clutching his chest, diaphoretic and pale, stating he had had sudden onset of substernal CP 30 minutes prior.
I looked at him and thought to myself: "this man is having an anterior MI". I almost activated the cath lab without an ECG, but we recorded one within 1 minute of arrival.
Here is that same ECG again:

I actually only saw lead V2 on the screen of the machine when I activated the cath lab. It had not yet even been printed out.
14 minutes later, just before going to the cath lab, the patient's pain went from 10/10 to 7/10.
Another ECG was recorded:
 |
| The T-waves in V2 and V4 are slightly smaller |
The patient went to the cath lab:
A large proximal LAD thrombus with TIMI-1 flow was found. Thus, there had been some minimal spontaneous reperfusion (autolysis). It was a wraparound LAD, explaining the inferior ST elevation with reciprocal ST depression in aVL (the opposite of what you expect with a proximal LAD occlusion). It was stented.
The post-cath ECG is here:
 |
| ST elevation is resolved. T-waves have normalized There is T-wave inversion in III with resolution of ST elevation. |
The cardiologists were not impressed by the ECG. This is the cardiology note:
"Pt's ECGs were not convincing but presentation was extremely concerning for ACS."
Summary
So this was an anterior and inferior STEMI due to an LAD that wraps around to the inferior wall. We do not see evidence of the ischemia of the first diagonal (which is distal to the occlusion and usually is revealed by STE in I and aVL). This is because that STE was cancelled out by reciprocal ST depression due to the inferior STE. The sinus bradycardia may be due to the inferior wall ischemia, although this happens primarily when there is occlusion of the RCA.
The 4-variable formula was correct.
The door to balloon time was 57 minutes.
This was recorded the next day:
 |
| Now there are Wellens' waves (terminal T-wave inversion), although with a poor R-wave. The poor R-wave suggests quite a bit of anterior infarction, probably permanent. |
Peak cTnI = 51 ng/mL
The echo next day showed:
The estimated left ventricular ejection fraction is 63 %.
Regional wall motion abnormality-distal septum anterior and apex akinetic
Regional wall motion abnormality-distal inferior wall .
Left ventricular hypertrophy concentric .
Regional wall motion abnormality-anterior akinetic.
Learning Points:
1. The pretest probability is important
2. R-wave amplitude is important
3. The 4 - variable formula is more accurate than the 3-variable
4. Look at the inferior leads.
5. Remember that a wraparound LAD can hide the findings of a proximal occlusion.